Evidence
I am sooooo overworked these days. So I'm doubling up on responsibilities. Today's post is actually a preview of my MicroSoft Small Business Forum column:
----

Recently, I attended a scholarly conference on the topic of evidence-based decision making. For those not in the know, "evidence" has been a hot topic in all areas of physical, medical and now social and political science for many years now. The idea is that one should base one's decisions on the best available information, rather than on other, presumably softer, criteria.
It might be surprising to many lay people to learn that Evidence-Based Medicine, or EBM, was fairly revolutionary when first introduced a few years ago. The assumption that most people make is that medical therapies, supposedly rooted in the rigour of Western science, is informed by clinical observations in controlled surroundings. For the most part, they are. But a large part of an individual doctor's decisions about his patient is also based on personal experience, or anecdote, and the personal experiences and hearsay of his teachers and colleagues.
The conference pitted two seemingly opposing viewpoints against one another. On one side was the hard science argument, that good evidence must always be at the core of decisions, especially decisions made by government in response to important phenomena, such as the appropriate policy responses to medical crises. The H1N1 pandemic is a good example.
On the other side was a proponent of the so-called "precautionary principle", which holds that sometimes it is not possible to wait for sufficient evidence to make a fully informed policy decision. Rather, sometimes it is incumbent upon policy makers to act within a milieu of great uncertainty.
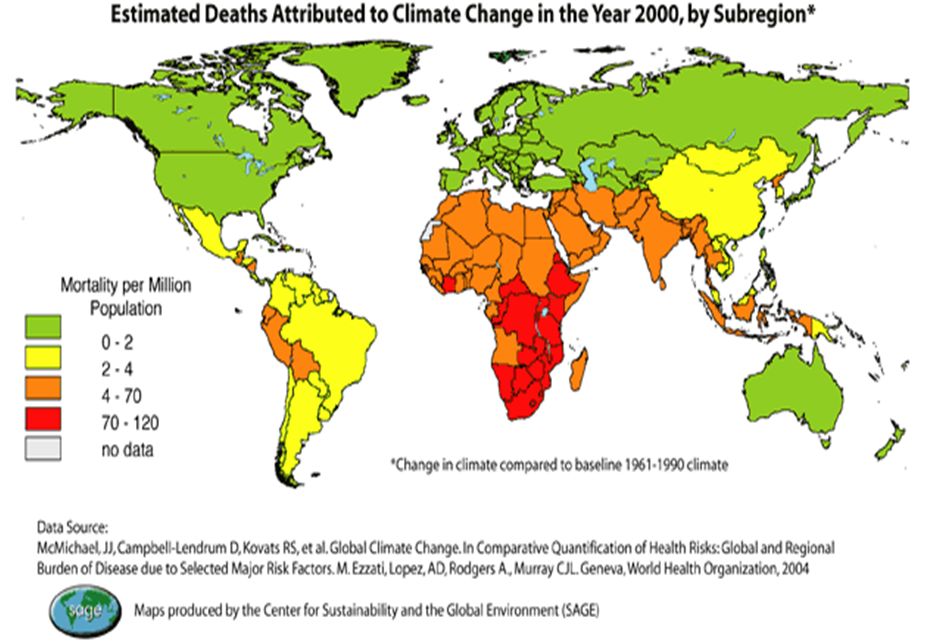
Arguments about the degree of evidence required to justify official action are themselves tainted by ideologies. Climate change is a good example. Those convinced that the phenomenon is real (and I count myself among that number) hold that the evidence is sufficiently convincing and the threat is sufficiently dire that the precautionary principle holds: we must act now and not wait until 100% are on side. The deniers would argue that we must wait until every last scientific hold-out is on-side.
But ultimately it is a false dichotomy. First of all, pitting "evidence" against the "precautionary principle" is misleading because the first involves a discussion about the nature of scientific rigour, while the second is a discussion of the nature of decision making.
Second, and most interesting to me, is that the discussion is ultimately a non-starter. Cynics (and again I count myself among them) would argue that decisions are almost never made with evidence prominently in mind. Rather, policies --especially those stated by governmental bodies-- are more likely to be informed by values, ideologies, politics and utility. Only after those avenues have been exhausted do decision-makers turn to the evidence, and then usually it is to justify a decision that has already been made.
I cannot estimate the extent to which this process is also prevalent in the business world, but I would not be surprised to find evidence getting short shrift there, either. But is this really a problem? I hope to explore this in a later segment.
----
Recently, I attended a scholarly conference on the topic of evidence-based decision making. For those not in the know, "evidence" has been a hot topic in all areas of physical, medical and now social and political science for many years now. The idea is that one should base one's decisions on the best available information, rather than on other, presumably softer, criteria.
It might be surprising to many lay people to learn that Evidence-Based Medicine, or EBM, was fairly revolutionary when first introduced a few years ago. The assumption that most people make is that medical therapies, supposedly rooted in the rigour of Western science, is informed by clinical observations in controlled surroundings. For the most part, they are. But a large part of an individual doctor's decisions about his patient is also based on personal experience, or anecdote, and the personal experiences and hearsay of his teachers and colleagues.
The conference pitted two seemingly opposing viewpoints against one another. On one side was the hard science argument, that good evidence must always be at the core of decisions, especially decisions made by government in response to important phenomena, such as the appropriate policy responses to medical crises. The H1N1 pandemic is a good example.
On the other side was a proponent of the so-called "precautionary principle", which holds that sometimes it is not possible to wait for sufficient evidence to make a fully informed policy decision. Rather, sometimes it is incumbent upon policy makers to act within a milieu of great uncertainty.
Arguments about the degree of evidence required to justify official action are themselves tainted by ideologies. Climate change is a good example. Those convinced that the phenomenon is real (and I count myself among that number) hold that the evidence is sufficiently convincing and the threat is sufficiently dire that the precautionary principle holds: we must act now and not wait until 100% are on side. The deniers would argue that we must wait until every last scientific hold-out is on-side.
But ultimately it is a false dichotomy. First of all, pitting "evidence" against the "precautionary principle" is misleading because the first involves a discussion about the nature of scientific rigour, while the second is a discussion of the nature of decision making.
Second, and most interesting to me, is that the discussion is ultimately a non-starter. Cynics (and again I count myself among them) would argue that decisions are almost never made with evidence prominently in mind. Rather, policies --especially those stated by governmental bodies-- are more likely to be informed by values, ideologies, politics and utility. Only after those avenues have been exhausted do decision-makers turn to the evidence, and then usually it is to justify a decision that has already been made.
I cannot estimate the extent to which this process is also prevalent in the business world, but I would not be surprised to find evidence getting short shrift there, either. But is this really a problem? I hope to explore this in a later segment.
Labels: epidemiology, science
posted by Raywat Deonandan at 10:36 PM
|
![]()